
Trending
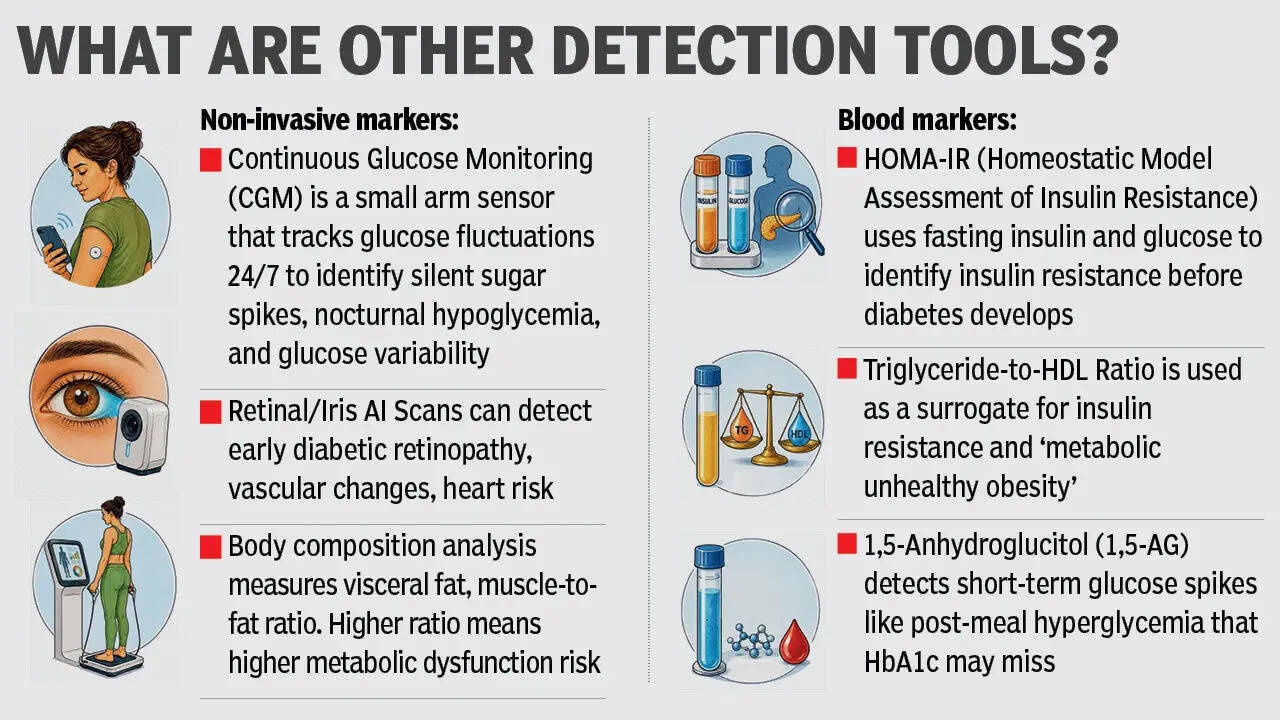
Diabetes clues your sugar test may miss

About the AuthorSteffy Thevar
End of Article
Follow Us On Social Media
Health +
Tired of too many ads?go ad free now
lifestyle videos
Featured In Lifestyle
Tired of too many ads?go ad free now

MORE FROM ETIMES
life & style
Hot on the Web
Shah Rukh KhanRanveer SinghKJR RajeshKangana RanautManoj BajpayeeBobby DeolGaurav GeraAhaan PandayBharat Bhhagya Viddhaata TrailerShilpa ShindeArchana Puran SinghKedarnath DhamParentingKheera VS KakdiDalchini Water BenefitsYash BhardwajProtein Powder RiskAnushka SharmaBarack Obama QuoteRakesh BediSpider Man Brand New DayDeepika PadukoneSalman KhanDrishyam 3 Box Office CollectionKaruppu Box Office CollectionPati Patni Aur Woh Do Box Office CollectionChand Mera Dil Box Office CollectionYashAjay DevgnHoroscope TodayDivorce DocumentsDelayed Chargesheet Kerala High CourtRudraM Surface MissileT-72 Tanks Digital MakeoverIAF France Jet DealHuman Evolving On Tibetan PlateauLargest Islands In The WorldJellyfish That Never DiesGoogle Release MosquitoesDelivery Firm Refund DeniedNyt ConnectionsCaptions For Instagram Posts
Trending Topics
Latest MoviesBollywood MoviesHollywood MoviesTamil Movies 2026Telugu Movies 2026Malayalam Movies 2026Kannada MoviesMarathi MoviesBengali Movies 2026Top Rated Movies 2026Best Hindi MoviesBest English MoviesBest Telugu MoviesBest Tamil MoviesBest Malayalam MoviesBest Kannada MoviesBest Bengali MoviesUpcoming Hindi MoviesBest Movies Of All TimeBest Hindi Movies of All TimeLatest English MoviesLatest Malayalam MoviesEnglish TV NewsTamil TV NewsTelugu TV NewsMalayalam TV NewsKannada TV NewsMovie ReviewsBhojpuri Cinema NewsGujarati Cinema News
Popular Categories
Viral NewsK Pop NewsWeb Series NewsAnime NewsUpcoming English MoviesUpcoming Tamil MoviesUpcoming Telugu MoviesUpcoming Malayalam MoviesUpcoming Kannada MoviesFashion TipsTravel NewsEntertainment NewsBollywood NewsTollywood NewsKollywood NewsMollywood NewsFood NewsLatest Hindi MoviesLatest Tamil MoviesParenting TipsHome RemediesWeight LossBeauty TipsParenting TipsHindi VideosHindi Video SongsBhojpuri Music VideosLatest Telugu MoviesBhojpuri Music VideoHindi TV News
Latest News
Hazaribag man drowns while fishing in lake"Behen Darr Gayi!": Fans relive ‘Bhagam Bhag’ era after watching Akshay Kumar's 'Bhooth Bangla' trailerMBOSE HSLC result 2026 to release tomorrow: Check details hereIran war risk: JPMorgan CEO Jamie Dimon warns of oil shocks, sticky inflation and higher interest ratesMake your clutch last longer with these easy driving tips“Three-against-one situation”: El Rubius opens up on being “targeted” in MrBeast’s viral $1M challengeBihar BTSC lab assistant notification released for 1091 posts at btsc.bihar.gov.in; apply hereIPL craze costs techie Rs 1.46 lakh in fake RCB vs CSK ticket scamRaising “robot-proof” kids: Why creativity and curiosity matter more than everInside ‘Satguru Sharan’: Exploring Saif Ali Khan and Kareena Kapoor Khan’s Rs 100 crore Bandra homeHow selling Alaska in 1867 was a costly mistake for Russia'Hera Pheri 3 is coming': Paresh Rawal dismisses delay reports and reveals he will 'start shooting soon'US-Iran War: A daring rescue Hollywood blockbuster is on its way. Till then, pick your favourite from these 10 films on bringing someone home against all oddsKolkata team unveils fan mural at Rash Behari Avenue, celebrating city’s first loveHow US spread a lie to rescue a pilot of a jet shot down in IranNetflix unveils ‘VOID’, an AI model that can change a movie plotAI data centers are causing 'stress' not just to tech companies, but also private insurers"Trans women are.....": Clavicular’s viral moment with trans women sparks fresh conversation on internet culture